The three-day long workshop brought together international expert physicians and scholars of Tibetan medicine – medical anthropologists, historians, (ethno)botanists, pharmacologists, pharmacists – working with and/or on Tibetan medicine, and also experts in Chinese medicine, as well as IT specialists. The aim was to discuss and contribute toward how an interdisciplinary and multilingual digital knowledge base should look like that could be used in the future as an analytic tool for documenting and analysing Tibetan medical formulas. Processes of cultural translation are intrinsic to such translations between different languages, medical concepts of health and disease, and disciplinary approaches and interests, and therefore are often vexed and problematic.
Prepared by a one-month-long pilot study by visiting scholar-physician of Tibetan medicine, Dr Cairang Nanjia from the Tibetan Medical College, Qinghai University, PRC, and the author of this report, at the time a Wellcome Trust research fellow at EASTmedicine, University of Westminster (2012-2015), this ensuing workshop proved a fruitful platform for discussing some of the outcomes and issues involved in such a complex endeavour. Both pilot project and workshop were co-funded by the British Academy/Leverhulme Small Research Grant combined with private funds by The Sino-British Fellowship Trust. Asian workshop participants were supported by an additional IASTAM fund. The author would like to express her gratitude to these foundations and to IASTAM that made this encounter between scholars from different disciplines truly special and fruitful. This included scholars who rarely discuss their different interests and approaches, physicians-cum-pharmacists from Asia, and pharmaceutical producers focusing on Tibetan formulas.
We focused on a particular Tibetan formula complex containing the main ingredient eaglewood (Lat. different types of Aquillaria; Tib. a ga ru or a gar)—in the following Agar-formulas (Agar 8, Agar 15, Agar 20, Agar 35, Sogdzin 11). These were chosen as case studies for they are usually prescribed in relation to specific classifications of ‘wind’ (Tib. rlung) disorders that can be correlated with what we understand as classic ‘stress’ symptoms, such as insomnia and depression.
Dr Cairang Nanjia began the inquiry by documenting Agar-formulas in Tibetan medical, botanical and pharmacological texts used at present in Amdo, the Tibetan populated parts of Qinghai and Gansu provinces of China, focusing also on their structure, single ingredients and relations to each other. The author related her ethnographic material on different styles of production and prescription practices of Agar-formulas in both China and parts of Europe, and both Cairang and Schrempf co-developed, together with advice from IT specialist Kapetanios a possible multi-level digital knowledge base structure of synonyms and homonyms in order to deal with the complexity of different languages, concepts and terminologies. The preliminary results were presented at the workshop for discussion.
Workshop participants used different sources and analysed them following up on specific questions, such as which texts are important for understanding Tibetan materia medica and formulae and by whom they are produced, prescribed and used today; which ingredients are we actually talking about in a formula; how and why are certain rare or endangered materia medica ingredients in a formula substituted; why and how does a formula work; what is its local, regional, botanical identification; what are ’wind’ (Tib. rlung) disorders in Tibetan medicine and how can one correlate them with biomedical diseases related to ’stress’ (let alone trying to define the fluid concept and the Tibetan dynamic of ’wind’, or what does stress mean to body and mind). Complex issues without doubt constantly required our own translation exercises between Tibetan, English and Chinese languages.
Sources used and topics addressed by the workshop participants ranged from analysing Tibetan historical medical and botanical texts to develop a feasible structure for Tibetan formulas (Czaja) to Chinese publications on minority medicines and how information on their materia medica is collected in China (Springer); how the seminal Tibetan medical text, the Four Tantras or rGyud bzhi explains the classification and treatment of rlung disorders (Cuomu); how specific rlung disorders, specially ‘heart wind’ (Tib. snying rlung) and ‘life sustaining wind’ (Tib. srog ’dzin rlung), are taught to Tibetan medical students in Xining (Sanjijia); presenting his experiences as a physician-cum-pharmacist by the eminent co-founder and teacher at the Tibetan medical hospital in Xining (Dr Nyima); how Agar-compounds in their various forms and styles are prescribed in both Asian and European contexts (Schrempf); presenting patient case studies and related prescription practices for ‘wind’ disorders in the UK (Millard) in which, however, no Agar-compounds were used; asking socio-cultural and ethno- as well as medical botanical questions about the difficulties in identifying plant names, such as Aquillaria agallocha (van der Valk, Allkin, Leon); demonstrating salient issues of sustainability of materia medica growing in Ladkah (Padma Gurmet); demonstrating the life work for Tibetan medicine by the eminent scholar and teacher Akong Rinpoche in both his home area of Kham and the UK, focusing on the sustainability of medical plants (Sweeney); how to understand Tibetan materia medica and formulas in relation to TCM while both address stress-related symptoms (Ploberger); how the pharmaceutical company Padma AG has created and adapted the Tibetan formula Sogdzin 11 into Padma Nervotonin (Schwabl and Vennos); and, last but not least, what a digital data base can offer if one is interested in mapping drugs across time and space (Stanley-Baker, Chen Shi-Pei, Brent Haoyang Ho).
The aim of the workshop was to relate and analyse formula and substitution patterns, culturally distinct ideas of efficacy and safety and different disease categories/body images in relation to ways of diagnosing, formulating/producing, prescribing and using these chosen Tibetan formulas. Only careful translations will allow to properly correlate different concepts of Tibetan, Chinese and bio-medicine, keeping regional, national and global regulatory regimes in mind. It would desirable if in the future we could pursue an integrative and synthesising approach to Tibetan Medicine with a sensitivity to various interpretations in this multi-lingual endeavour, as well as trying to correlate different disciplines and practices.
The aim would be to explore careful and meaningful ways of representing Tibetan cultural and medical knowledge and develop suitable key search terms in different semantic networks in order to make such a digital knowledge base a useful tool for researchers and practitioners alike.
Syndicated Post By Nomin Galsandorj. This post first appeared at http://theubpost.mn/2016/08/03/mongolian-traditional-medicine/
Traditional systems of medicine in countries such as Nepal, Sri Lanka, Bangladesh, Pakistan, Tibet, and Mongolia appear to be derived from Ayurveda. In Indian, Tibetan, and Mongolian traditional medicine, the mind, emotions, and body are not seen as separate but as a continuum. A person’s emotional and mental states are seen as having a significant impact on the body and vice versa. Mongolian, Tibetan, and Indian traditional medicine use a number of modalities or therapies for both prevention and treatment of disease. Many medicinal herbs are usually used in combination.
Mongolia has a severe climate with four seasons, throughout which nomadic Mongolians move from place to place tending to their domesticated animals. Their way of life and medical treatments are very peculiar. The methods of medical treatment are derived from their simple lives. Medicinal herbs, the limbs of animals, and minerals are used as natural forms of medical treatment. They are sometimes used individually and sometimes used together for
medicinal purposes. Mongolians combine medicine with psychological therapy and use sayings, such as mantras, shamanic charms, and prophecy. There are certain influences of Buddhism in Mongolian medical treatment, such as the use of spells and the stating of one’s requests and mantra expressions.
In the 4th and 5th centuries, monks of Tibet, Nepal, and China were studying Buddhism in India, and it provided the opportunity for Buddhism to spread in Tibet. Medical books from India were translated from Sanskrit into Tibetan. When Mongolia tried to make Buddhism the official religion in the 13th century, Indian and Tibetan medical books came to Mongolia as well.
The book “Four Tantras” (Jud Shi) was written in the 11th century, a classic creation of Indian and Tibetan medicine. “Jud Shi” was the main textbook of Mongolian doctors when it arrived in the 14th century. In Mongolia, it was read in Tibetan and was also translated into Mongolian. The Mongolian version has been published many times. German scholar Walther Heissig wrote that Choiji Odser translated “Jud Shi” in the 14th century, and during Ligden Khan’s time (1604-1634), “Jud Shi” was revised and re-translated.
The five elements theory of Indian philosophy started to hold an important position in the basic principles of Mongolian traditional medicine and this is related to the popularity of “Jud Shi” in the 16th century and its translation into Mongolian. “Jud Shi” is the amalgamation of Tibetan and Mongolian medicine and the Indian sutra.
“Jud Shi” has four volumes, identified by tantra:
1. Basic Tantra- The Basic Tantra has four parts and is the basis of the other three tantra volumes. It contains all the general meanings of the Four Tantras and is a basic overview of the theories of Indian and Tibetan medicine.
2. Explanatory Tantra – This tantra has 31 parts. The root of Indian and Tibetan medicinal
theory is defined briefly here.
3. Oral Instruction Tantra – This tantra has 92 parts and is the largest part of the book. It
describes how diseases and disorders of the body and organ systems are generally understood in Indian and Tibetan medicine.
4. Subsequent Tantra – This tantra has 27 parts and draws conclusions on the therapies in
the other 3 volumes.
Medicine Buddha by G.Zanabazar
In the 18th century, Mongolian scholar Gombojav was the primary translator of “Dankhaivjunai”, a large Tibetan-Mongolian dictionary, and participated in the Mongolian translation of “Danjuur”. The book “Medicinal Formulas”, which was written by Gombojav, was block printed in Mongolian. In the book, he included some formulas from Indian, Tibetan, and Khoton medicine.
Jambaldorj was one of the greatest doctors in Mongolia during the 19th century. He wrote a 174-page sutra called “Zetsermigjan”. During this time, there were errors and mistakes in identifying medicinal ingredients. He researched the work of the best ancient doctors of India, Tibet, and Mongolia, and defined the shape, form, features, and potency of the medicinal ingredients used. He also wrote a book about ingredients in Sanskrit, Tibetan, Chinese, Manj, and Mongolian, complete with 576 images. This book has attracted the attention of national and foreign scholars and has been published in foreign countries.
Luvsanchultem was a Mongolian doctor of the 19th century. He wrote about the Indian “five elements” theory used in Indian and Tibetan medicine. Mongolians enriched the ancient books on medicine that were passed on from India to Tibet. In Mongolian traditional medicine, anatomy, diseases, and the effects of medicine are explained on the basis of the five elements theory.
Five elements theory and three types of combinations
The five elements theory and the three types of combinations of these elements are the main parts of Indian, Tibetan, and Mongolian traditional medicine. Everything in the universe, including human beings, is composed of five basic elements. The five elements are earth, water, fire, air, and space. These five elements form the metabolism of the body.
– Earth controls the physical structure of the body: bones and flesh. All life forces become
inert and inactive in this element and more energy is used to keep a body active.
– Water controls the kidneys, male and female reproductive organs, and produces antibodies. Water keeps the body and life flowing.
– Fire controls the spleen, liver, pancreas, and keeps all the organs active. It creates fire in the body. It heats water. It regulates sight, provides strength to the body by digesting food, induces hunger and thirst, maintains the suppleness of muscles, and a beautiful complexion.
– Air controls the chest, lungs, and heart and forms the purity of the mind and heart. Air is life itself. It is strength and guides every part of our body. It moves bile and phlegm, which cannot move in the body by itself.
– Space controls the entire body, thyroid, parathyroid, tonsils, saliva, cerebral and spinal fluid, the nervous system, and eliminates poison from the body. In order for air to circulate in the body and maintain a proper balance, there has to be space. If such circulation is blocked, it creates pain, even leading to heart attacks and loss of consciousness.
All these elements should be maintained in proper proportions. Any disturbance (and excess or deficiency) of one element leads to disturbances in other elements, and is considered the root cause of disease. If these five elements are maintained in proper proportions in the body, a proper metabolism is ensured and the body remains healthy. However, due to heredity, as well as eating and living habits, we can disturb one or two of these elements and upset the metabolism. When there is an illness present there is a predominance of one or more of three types of combinations of the five elements. In Indian, Tibetan, and Mongolian traditional medicine, people are diagnosed as being one of these three types of elemental combinations.
1. Kapha (Bad-kan) – the combination of excessive earth and water These elements occupy the largest areas of our body. Kapha people have a regular appetite with relatively slow digestion, and prefer warm drinks and like pungent, astringent, and bitter foods.
2. Pitta (Tri-pa) – the combination of excessive fire and air Pitta people have a strong metabolism, and a good appetite and digestion. They like large quantities of food and water, and like bitter, sweet, and astringent foods and cooling drinks.
3. Vata (Lhung) – excessive air Vata people have a variable appetite and crave salty, sweet, and sour foods, and prefer warm or hot drinks. Their hands and feet are usually cold and dry with cracked skin.
In Indian, Tibetan, and Mongolian traditional medicine, all foods are divided into six tastes: bitter, astringent, pungent, sweet, sour, and salty.
Mongolian diet therapy
Mongolians eat the following five kinds of food:
White – dairy products
Red – meat products
Green – plants and vegetables
Yellow – butter and oil
Black – water and distilled milk vodka
The five kinds of food of the Mongols include milk and milk products, such as curds, fermented mare’s milk, clotted cream, butter, sea buckthorn oil, cedar nut oil, apricot oil, and sheep tail fat.
The oil from sheep tail fat contains calcium, magnesium, iodine, and fluorine. It is also rich in vitamins D, C, A, K, E, B, and is good for fatigue, allergies, poisoning, and the eyes. Sheep tail fat has many medicinal qualities and is very nutritious, and has been considered beneficial “food” for infants and elders since ancient times. It enhances the metabolism and digestion, provides energy, prevents weakness and fatigue, and is thought to speed up the growth of infants. It moisturizes, softens, regenerates, and rejuvenates the skin. Sheep tail fat contains nutrients that cannot be found in any other food. The tip of the sheep tail, which is called uurag suul, is the best nourishment for the liver and supports the brain.
In Mongolian traditional medicine sutras, it’s written, “Fresh white butter is of cool quality and cures lung diseases and coughing, and treats fever. Old butter cures mental disorders, hangovers, and diseases of the eyes, brain, and womb.” In ancient sutras, it’s written “Yellow butter kept for years is good at treating diseases when applied to the skin. It has many diverse curative qualities if mixed with other ingredients. Yellow butter enhances intellectual capability, relaxes the mind, and refreshes one’s sight. It makes elders younger and makes voices melodious. It also improves fertility and cures diseases of the ears, lungs, and mind, and burns, frozen wounds, or cold weapon injuries.” The sutras also say, “Cow’s milk butter is very nutritious and good at healing any illness. The butter of goat’s milk is of cool quality and treats fevers. Yak or sheep milk is of hot quality and produces energy.”
In Indian, Tibetan, and Mongolian medicine, it is said, “Unsuitable food is poison to one’s body. Perfect food nourishes and keeps the body fit, healthy, and energetic. If the food is too little, the body weakens, beauty fades, and illness appears. If the food is too much, the body gets tired from over-consumption and is invaded by sickness. Thus, two quarters of the stomach should be full of food, one quarter of drink, and one quarter left empty.”
Nomadic Mongolians had a healthy lifestyle. During the winter time, meat products were mainly eaten, and during the summer time, dairy products, vegetables, and fruits were mainly eaten. The four conditions of climate, evil spirits, diet, and lifestyle act together to affect disorders. The four remedial measures for disorders are diet, lifestyle, medicine, and external therapies.
The following disorders are treated in Indian, Tibetan, and Mongolian traditional medicine: hot and cold disorders, pediatric disorders, gynecological disorders, wounds, geriatric disorders, infertility, indigestion, tumors, edema, fever, smallpox, and the common cold. They also treat disorders of the head, the eyes, the ears, the nose, the mouth, the goiter, and genital disorders; disorders of vital vessels and organs, such as the heart, lungs, liver, spleen, kidneys, stomach, intestines, and colon. Miscellaneous disorders, such as laryngitis, anorexia, hiccups, asthma, vomiting, diarrhea, constipation, diabetes, gout, arthritis, skin diseases, nervous disorders, and minor injuries are also addressed.
For centuries, Indian, Tibetan, and Mongolian medicinal practices were used not only to diagnose diseases but also to prescribe medicine based on individual conditions, using a unique system of evaluating the pulse, eyes, tongue, skin, and smell. The botanical formulas used thousands of years ago continue to be in use today. The Indian, Tibetan, and Mongolian traditional medicine systems are fond of using formulas involving multiple herbs.
The treatments include decoctions, powders, pills, paste, medicinal butter, calcinated powder, gems, herbal compounds, oil therapy, purgation, emesis, nasal drops, enemas, channel cleansing, venesection, moxibustion, cauterization, compression, medicinal baths, natural spring baths, massage, and surgical therapy.
The diagnostic techniques are visual study, pulse taking, and interrogation. The visual study involves the examination of the tongue and urine. Touching with the fingers is like receiving information transmitted by the patient’s pulse. Interrogation involves the patient’s medical history, looking at the signs and symptoms of illness, as well as dietary factors.
For centuries, Mongolians have utilized traditional methods for surviving the harsh winter season. During the winter months, Mongolians eat “hot” foods that are rich in vitamins and minerals, and abstain from eating “cold” foods. Eating hot foods has the positive effect of increasing blood flow, energy level, improving the functions of the main organs of the body (including the digestive system), and has been scientifically proven to prolong life expectancy to an average of 70 years. However, in recent years, the life expectancy of the population has been decreasing, due to improper dress during the winter season and spending too much time in cold places, therefore not being able to maintain internal body heat. The long-term effect of this is a decrease in the immune system’s functions, cold sweats, and lower blood levels. Daily consumption of cold starters and salads, coffee, soft drinks, juices, beers, and other drinks that are below room temperature and straight from the refrigerator can lead to “cold” digestive ailments.
Cold water, drinks, and ice cream reduce body heat and increase the burden placed on the digestive system. In Indian Ayurvedic medicine, it is said that heat is life, while cold is death. Due to these practices in recent years, and particularly among young people, intestinal inflammation, stomachaches, stomach ulcers, the feeling of fullness or bloating, constipation,
and the removal of gall bladders have been much more common.
Yellow Pasqueflower, commonly used in traditional medicine
Mongolia is home to hundreds of rare medicinal plants, most of which are found in the Khangai Mountain Range and the steppes. Prior to making any traditional medicine, plants must be collected at the appropriate time or season. For instance, the yellow snowdrop (aneta) blooms in early spring. Therefore, the exact time of its full bloom must not be missed and the collected plants should be dried out.
There are cases where toxic vegetation is used to make medicines. Those toxic plants need special care, and there are specific methodologies for drying and removing the plant’s poison. A branch of a toxin-containing tree must be cut in half before drying. If the plant has a poisonous surface, the outer layer must be scraped away. To release the toxins in spar, it needs to be placed in a covered dish and set on fire.
Indian, Tibetan, and Mongolian traditional medicine is based on a philosophy that guides the practitioner to serve his patient according to special needs at a special time, and under special circumstances. They are extremely individualized, personal, and flexible, dependent on a person-to-person and expert-to-client relationship. Treatments and prescriptions are tailor-made for the patient, and take into account the individual’s constitution, age, gender, syndrome, primary complaints, accompanying signs and symptoms, the season, and the geographic location.
Nomin Galsandorj is a freelance writer and translator, translating texts from English to Mongolian, including the Dalai Lama’s official website. She can be contacted at nomin1994@yahoo.co.uk.
This three-day workshop (May 8-10, 2015) at EASTmedicine, University of Westminster, London brought together international expert physicians and scholars of Tibetan medicine – medical anthropologists, historians, ethno- and medical botanists, pharmacologists – working with and/or on Tibetan medicine, and also experts in Chinese medicine as well as IT specialists. Organised by Mona Schrempf, the author of this report, the workshop was funded by the British Academy/Small Leverhulme Research Grant, the Sino-British Fellowship Trust and IASTAM (International Association for the Study of Traditional Asian Medicine). It had the aim to discuss and contribute to what an interdisciplinary and multilingual digital knowledge base should look like that could be used in the future as a tool for documenting and analysing Tibetan medical formulas for a variety of scholarly users worldwide, including physicians of Tibetan medicine working in many different national contexts in Asia and the West.
Such an ambitious endeavour requires complex processes of re-translation and re-contextualisation of and between Tibetan medicine and biomedicine (and partly Chinese medicine) in the relevant languages Tibetan, English, Latin, and Chinese, and also between different disciplines involved. Therefore, we focused on a common global ailment of our time that many of us universally suffer from – stress. We approached the topic from different angles, starting with a set choice of multicompound Tibetan formulas containing as main ingredient eaglewood. They are prescribed for specific types of ‘wind’ (Tib. rlung)[1] disorders in Tibetan medicine that are characterised by common stress symptoms – insomnia, restlessness, lack of concentration, light depression. ‘Wind’ is the principle of movement within the body and governs the functions of thought, breathing, and other physical movements, such as bowel movement, etc. in Tibetan medicine. Stress-related ‘wind’ disorders are usually caused by and located in or around the heart, i.e. by an imbalance of the ‘heart wind’ (Tib. snying rlung) or the ‘life-sustaining wind’ (Tib. srog ’dzin rlung).
Such ‘wind’ disorders are generally treated – next to using other treatment methods (nutrition, behaviour, massage, moxibustion) – with a specific set of Tibetan formulas containing as main ingredient eaglewood or agar wood (Lat. different types of Aquilaria; Tib. a ga ru or a gar)[2], in the following shortly called Agar-formulas (Agar 8, Agar 15, Agar 20, Agar 35, Sogdzin 11). Eaglewood is both a potent medicinal and fragrant resinous wood, also used in medicinal incense against insomnia (Agar 31). Its use is problematic because of the unresolved botanical identification of Aquilaria malaccensis that is endangered and CITES-listed[3]. Nevertheless, Agar-formulas are very popular and frequently prescribed in Tibetan medicine. They are produced and prescribed as compounded formulas by physician-cum-pharmacists or by physicians administering readily manufactured pills; however, they might be also directly taken as a dietary supplement.
We looked at different Agar-recipes and their various formulations, their ingredients and indications. At the workshop, Tibetan scholars also presented classical Tibetan medical texts and certain pharmacopoeias used for producing these formulas. It quickly became evident, however, that both the complexity of different disease categories and understandings of causes of illness in Tibetan medicine are not easily translatable into European biomedical or even ‘alternative medical’ understandings. On the other hand, it is possible and practiced already. Researchers at one pharmaceutical company in Europe producing Padma Nervetonic based on the Tibetan formula Sogdzin 11 explained at the workshop how and why they had to adapt or omit certain ingredients of the original formula which is administered for stress to European patients, how its overall efficacy is maintained and understood, as well as proven and regulated within European frameworks of production and distribution (on such a process of translation, see Schwabl and Vennos 2015).
Processes of cultural translation are intrinsic to correlating and making sense of illness and treatment between different languages, of medico-cultural concepts of health and disease, and of various disciplinary approaches and interests, yet they are vexed and problematic and therefore often ignored or glossed over. We tried to do the opposite in this workshop by carefully translating together the same formulas from different disciplinary perspectives and retranslating ‘in-between’ those. Prepared by a one-month pilot study by visiting scholar-physician of Tibetan medicine, Dr Cairang Nanjia from the Tibetan Medical College, Qinghai University, PRC, and the author of this report, Mona Schrempf – at the time Wellcome Trust Research Fellow at EASTmedicine, University of Westminster (2012-2015) – this ensuing workshop proved a fruitful platform for discussing some of the outcomes and issues involved. It is hoped that the initial results from this workshop will serve as a basis for future international research cooperations on the topic of Tibetan materia medica and formulae (Schrempf forthcoming a,b).
Our pilot-study examined Agar-formulas based on their original recipe texts and documentations as well as different application contexts in China and Europe. From a Tibetan medical point of view, it is impossible to narrow down the efficacy of a particular formula or even of a single ingredient within a formula to one specific disease only (usually defined in biomedical terms). Rather than perceiving this gap in translation between different medical principles as a loss, it can also open up a space for research examining how careful correlations between different medical principles can allow for a more complex and complete view of disease in relation to a particular formula, and maybe even shed light on possible causes and explanations on how disease can originate. Tibetan formulae are conceptualised in a way that they balance internally the different efficacies of single ingredients as to avoid side-effects while multitargeting connected imbalances in the body.
Traditionally, Tibetan formulae are not only prescribed for a particular imbalance in the body but individually according to the constitution of an individual patient and according to the stage of a disease or combination of disease(s), etc. For this subtle individual prescription, pulse diagnosis is necessary. It is the only way to know which particular imbalances are present or dominate and therefore in need of immediate treatment within a patient’s body. So how can this aetiological and epistemological complexity be translated into a fixed biomedical disease entity required to prove biomedically defined efficacy that is, for example, necessary for producing industrialised, quality approved and licensed pharmaceuticals? This is just one of the many questions of translation that we were addressing in this workshop[4].
The individual workshop presentations
Cairang Nanjia (Tib. Tsering Namgyal) began by documenting Agar-formulas in Tibetan medical, botanical and pharmacological texts used at present in Qinghai, China. He was focusing on the structure of the formulas, comparing the single ingredients and their relations to each other. We also looked at the different translations of these formulas into Chinese and English as well as German languages and prescription leaflets, adaptations that were sometimes also altering the actual composition of the formulas. The author of this report, Mona Schrempf, related her ethnographic material on different styles of production and prescription practices of Agar-formulas in both China and parts of Europe (Schrempf, in press, forthcoming a). With the advice from IT specialist Kapetanios, Cairang and Schrempf developed a possible multi-level digital knowledge base structure of synonyms and homonyms in order to deal with the complexity of different languages, concepts and terminologies connected with the Agar-formulas in an adequate way using different disciplinary approaches as access points to the digital knowledge base envisioned. The preliminary results were presented at the workshop for discussion and have benefitted, among others, specifically from the input by Bob Allkin, IT-specialist for digital Plant Names Services at the Royal Botanic Gardens Kew, London. He explained why plant names matter and how he organises Kew’s digital knowledge base using authoritative international naming and taxonomic resources, what the obstacles are for appropriate naming and use, how things can go wrong, and the role of the food and drug administration in deciding what is toxic and what not.
Workshop participants used different sources for looking at the Tibetan Agar-formulas and analysed them following up on specific questions, such as: Which texts are important for understanding Tibetan materia medica and formulas produced today? Who produces these formulas using what kind of knowledge and production technology, and how is this connected to (biomedically defined) efficacy and safety issues? Which ingredients are we actually talking about in a specific formula and how do we identify them botanically while addressing their regional diversity at the same time? How and why are certain materia medica ingredients in a formula substituted? How does a formula work and for what kind of disorders, related to which organs etc.? How can we understand ‘wind’ (Tib. rlung) disorders in Tibetan medicine correctly, and in particular, ‘heart wind’ and ‘life-sustaining wind’ treated by Agar-formulas? Is a translation between these specific wind-disorders and what we call ‘stress’ possible at all? Is it effective to prescribe an Agar-formula for stress symptoms without a prior detailed pulse diagnosis of the individual constitution of the patient and his or her specific disease by a physician of Tibetan medicine?
These are complex issues without doubt that we tried to address by re-translating between Tibetan, English and Chinese languages and inherent health and disease concepts in Tibetan and biomedicine as well as – at least where China is concerned – also in relation to Chinese medical concepts. The latter appear on package leaflets of Tibetan medicines in China, written in Chinese. Sources used and topics addressed at the workshop ranged from analysing Tibetan historical medical and botanical texts for developing a feasible structure for Tibetan formulas (Olaf Czaja) to Chinese publications on minority medicines and how information on their materia medica is collected in China (Lena Springer); how the seminal Tibetan medical text, the Four Tantras or rGyud bzhi explains the classification and treatment of rlungdisorders (Mingji Cuomu); how specific rlung disorders, specially ‘heart wind’ (Tib. snying rlung) and ‘life sustaining wind’ (Tib. srog ’dzin rlung), are taught to Tibetan medical students in Xining (Sanjijia); and what the experiences with treating rlung disorders at the Tibetan medical hospital in Xining are, demonstrated by the eminent 84 year old co-founder, teacher and physician-cum-pharmacist, Akhe Nyima.
Colin Millard presented patient case studies and related prescription practices by Lobsang Dhonden Soktsang for ‘wind’ disorders at the Tara Clinics, UK, in which, however, no Agar-compounds were used. IT-specialist Bob Allkin and medical botanist Christine Leon from the Royal Botanic Gardens Kew gave stunning presentations of the complexity of identifying just one single plant in a botanically correct way. In contrast, the ethno-botanist van der Valk asked questions on whether the fixation on a specific botanical identity of, for example, ‘eaglewood’, does not counteract or limit the diversity and regional flexibility of this particular medicinal plant.
This flexibility is also connected with the sustainability of these plants used in many Tibetan formulas whose ingredients mostly grow in the wild in the Himalayas and on the Tibetan Plateau – and are often locally not accessible for small scale producers, such as private physician-cum-pharmacists. Padma Gurmet from the Sowa Rigpa Institute in Ladakh demonstrated the ongoing efforts to cultivate and sustain medicinal plants growing in the wild in Ladkah. Brion Sweeney demonstrated the important work by the eminent scholar and teacher Akong Rinpoche in both his home area of Kham and the UK for Tibetan medicine focusing on the sustainability of medical plants and Tibetan medical education. Florian Ploberger discussed the Tibetan materia medica of Agar-formulas from the point of view of TCM-phytotherapy. Herbert Schwabl, director of research at Padma AG, and Cecile Vennos, head of regulatory and medical scientific affairs, explained how they had adapted the Tibetan formula Sogdzin 11 into becoming Padma Nervotonin (Schwabl & Vennos 2015). Last but not least, Michael Stanley-Baker, Chen Shi-Pei, and Brent Haoyang Ho from the Max Planck Institute for the History of Science, Berlin, explained what a digital data base can offer if one is interested in mapping drugs across time and space.
Perspectives
The aim of the workshop was to sound out what kind of information is important in order to fully document and analyse Tibetan medical formula in a multidisicplinary and multilingual digital knowledge base. Only careful translations will allow to properly correlate different concepts used and applied to these formulas, from Tibetan, Chinese and bio-medical knowledge, the impact of regulatory regimes on the formulas in each national context. It would be desirable if in the future we could pursue an integrative and synthesising approach to Tibetan Medicine with a sensitivity to various interpretations in this multi-lingual endeavour and one which adequately represents the varying involved disciplines and therapeutic practices. The aim would be to explore careful and meaningful ways of representing Tibetan cultural and medical knowledge and develop suitable key search terms in different semantic networks as to make such a digital knowledge base a useful tool for researchers and practitioners alike.
[1] ‘Wind’ or loong (rlung) in Tibetan is one of three complex bodily principles in Tibetan medicine, the other two being ‘bile’ or tripa (Tib. mkhris-pa) and ‘phlegm’ or peken (Tib. bad-mkan), resembling Ayurvedic principles with which they are historically connected. An imbalance of these three bodily principles causes disease. For more information, see http://tibet-medicine.org/de/tibetische-medizin/grundlagen/die-grundprinzipien/
[2] One of the problems we are facing is the botanical identification and regional variety of this plant. It can be, for example, Aquilaria agallocha Roxb., Aquilaria sinensis, Cinnamomum pharthenoxylon Tack.
[4] Medical anthropological research publications on Tibetan medicine alias Sowa Rigpa (Tib. gso ba rig pa), the ‚Science of Healing‘, mainly as practiced in Asia, are growing. See Adams, Schrempf & Craig 2010; Blakie 2013, 2015; Craig 2012; Janes 2002; Hofer 2012; Kloos 2013; Pordié 2008; Saxer 2013, Schrempf 2007, in press, forthcoming a,b.
References
Adams, Vincanne, Mona Schrempf & Sienna Craig (Hgs). 2010 (2013). Medicine Between Science and Religion – Explorations on Tibetan Grounds. London, New York: Berghahn Publishers.
Blakie, Calum. 2013. Currents of Tradition in Tibetan Medicine Pharmacy. In: East Asian Science, Technology and Society 7 (3), 425-451.
—— 2015. Wish-fulfilling Jewel Pills: Tibetan Medicines from Exclusivity to Ubiquity. In: Anthropology and Medicine22 (1), 7-22. DOI: 10.1080/13648470.2015.1004504
Craig, Sienna. 2012. Healing Elements: Efficacy and the Social Ecologies of Tibetan Medicine. Berkeley: University of California Press.
Janes, Craig. 2002. Buddhism, Science, and the Market: The Globalisation of Tibetan Medicine. In: Anthropology and Medicine 9 (3), 267-289.
Hofer, Theresia. 2012. The Inheritance of Change. Transmission and Practice of Tibetan Medicine in Ngamring. Wien: Arbeitskreis für Tibetische Buddhistische Studien Universität Wien, Wiener Studien zur Tibetologie und Buddhismuskunde, Heft 76.
Kloos, Stephan. 2013. How Tibetan medicine in Exile Became a „Medical System“. In: East Asian Science, Technology and Society 7 (3), 381-395.
Pordié, Laurent (Hg). 2008. Tibetan Medicine in the Contemporary World. Global Politics of Medical Knowledge and Practice. London & New York: Routledge.
Saxer, Martin. 2013. Manufacturing Tibetan Medicine. The Creation of an Industry and the Moral Economy of Tibetanness. Oxford, New York: Berghahn Publishers.
Schrempf, Mona. 2007. Soundings in Tibetan Medicine. Historical and Anthropological Perspectives (Proceedings of the 10th Seminar of the International Association for Tibetan Studies (PIATS), Oxford 2003). Leiden: Brill Academic Publishers.
—— (2015, in press). ‘Formulation Regimes and Styles of Practice in Transnational Tibetan Medicine – a Comparative Perspective on Efficacy and Safety between China and Europe. In: Mona Schrempf & Lena Springer (Hgs). Efficacy and Safety in Tibetan and Chinese Medicine: Historical and Ethnographic Perspectives (special issue) Asian Medicine – Tradition and Modernity 10 (1-2), 35 p.
——(forthcoming a) A Tibetan Medical Root Formula and its Derivatives: Cultural Translations in Transnational Styles of Practice.
——(forthcoming b) Transnational Tibetan Medicine – Formula Regimes, Therapeutic Networks and Styles of Practice between China and Europe (Berghahn Publishers)
This is a syndicated post that first appeared at savageminds.org
Only those who regard healing as the ultimate goal of their efforts can, therefore, be designated as physicians. —Rudolf Virchow
When Gyatso called to give me the list of medicines I was in the library, writing another one of these blogposts. I answered his call, speaking as quietly as I could in Tibetan but hoping he would still be able to hear me, across the planet. A few students looked up, annoyed, as my weird banter broke their concentration. Once outside, I greeted this familiar voice with enthusiasm. Gyatso, a Tibetan doctor or amchi with whom I have worked for many years, was calling from his home in the ancient walled city of Lo Monthang, in Nepal’s Mustang District.
Pleasantries passed and then Gyatso got down to work. Do you have a pen and paper? He asked. I pulled out my notebook and he began to rattle off the names of about 30 different Tibetan medical compounds. Most I recognized as common formulas with as few as five and as many as twenty-five ingredients: plants, animal products, and minerals from across the Tibetan plateau, high Himalaya, and subtropical South Asia. As I wrote down these names, sensory memories flooded in, of dried pomegranate and green cardamom, of eaglewood and Chinese gooseberry, of calcium carbonate and bamboo pitch. The names of these formulas also brought forth a string of symptoms: sleeplessness and anxiety, blood and bile disorders, digestive irregularities, weakened life force. A few of the named medicines were rinchen rilbu, precious pills. These highly complex pharmacological endeavors include detoxified precious and semi-precious stones and metals. They are used sparingly, if also as panacea.So as not to fully deplete Gyatso’ own medical supplies, with which he treats his own rural community, I had brokered donations of Tibetan medicines from a reputable doctor with her own small pharmacy in India. The doctor would package up this precious cargo and send it by bus from Delhi. Gyatso, along with his brother, heads up a school and medical clinics in Mustang and Pokhara. He was beginning to mobilize several of his senior students along with a few local youths who would then head to the Village Development Committee from which one of their former students and the cook at their school hails: a region in Dolakha District that was severely damaged in the April 28 quake and then further impacted by the May 12 event. After some initial questions about where they should go, they decided on a closely hewn response: help those you know, or those you can trust to help you reach people they know. This sort of practical wisdom turns stereotypes about Nepali propensities to privilege ‘one’s own people’ (aphno maanche) on its head.
As our conversation continued, the structure and form of what will likely be the first of several Amchi Medicine Clinics to emerge in response to the Nepal earthquakes took shape. These clinics aim to provide not only Tibetan medicines and food but also to offer support through ritual practice to honor the dead and protect the living. The idea for these camps was suggested by various amchi soon after the first earthquake. Although their strategies regarding where and when to and who to send go varied, these practitioners presented a single-pointed vision when it came to the purpose of such an endeavor. They would provide culturally astute, mindful care for people living with and suffering from forms of embodied trauma that can be well served by this medical tradition. They understood that without enough to eat, medicines would bring less benefit. They knew that people would value the lighting of butter lamps, but would not necessarily have the butter to offer. The anticipated ongoing physical trauma from the work of dismantling homes but also the needed work of clearing away the spiritual pollution evoked by so many violent, untimely deaths. They spoke of the need to appease local deities of place and to reconsecrate damaged structures.
A Nepali amchi diagnosing a patient through pulse analysis. Photo credit: Joan Halifax
Most of all, what has taken clinical psychiatry and international disaster response teams many years – and many disasters – to understand came easily for them. The awkward hyphens of bio-psycho-social meld into a different social ecology of health and illness for these practitioners, one that takes seriously the reality that the elements which make up this planet are also those which give us sentience: earth, air, fire, water, space. Amchi are at once ethnobotanists and ritual specialists attune to the living landscapes and sacred geographies of home as well as pharmacologists and physicians. The modes of knowledge transmission they represent might be considered critically endangered in an era of ‘big’ traditional pharma as well as the introduction of biomedically-derived production standards and clinical research protocols, but they know how to respond in meaningful ways at such moments of crisis. They also understood that they could perhaps be most helpful not in the immediate rescue and triage mode but in response to the settling in of suffering over these coming months, when time stretches out into new spaces of vulnerability, memory, loss.
Non-biomedical health systems and various forms of traditional medicine remain a crucial avenue through which many Nepalis seek care for chronic and acute illness, including mental health and responses to trauma. Nepalis rely on Tibetan medicine to address their health concerns, both in rural villages along Nepal’s northern border and in urban clinics, where patients represent Nepal’s ethnic and cultural diversity. Also known as Sowa Rigpa, the ‘science of healing,’ this medical practice is less formally recognized and supported by the Nepali government than Ayurveda, even as amchi work at the frontline of care for many of the country’s high mountain communities.
As Nepal’s amchi move forward with their planning, they will work closely to coordinate with other relief organizations working in these areas. Their aim is not to reproduce the infrastructure of aid delivery but to connect directly to such efforts while providing distinct forms of care. I hope that such efforts by highly skilled Tibetan medical practitioners might dissuade – or at least provide a counter-example to – those biomedical aid workers who have decided that it is acceptable to just pluck up some traditional medicines and, with rudimentary translation of symptoms and no training in proper diagnostic methods (pulse and urine analysis) or understanding of the clusters of imbalance such medicines are meant to address, hand them out to people anyway. This is another form of biomedical hubris and a certain type of cultural violence, seeping in around the edges of right motivation. Imagine the pushback if a Tibetan physician were to show up in an emergency room and begin prescribing anti-psychotics and blood thinners, willy nilly.
Although these amchi medical clinics are proposed within an ephemeral ‘camp’ structure at present, such effort may represent an opportunity to re-imagining post-quake healthcare infrastructure in ways that more directly incorporate practitioners such as amchi into the provision of primary health care. The foundation for such work exists, as amchi are marginally recognized (if not supported by) Nepal’s Department of Ayurveda within the Ministry of Health, and through the Council on Technical Education and Vocational Training. Full-scale support for and integration of amchi into public health infrastructure remains a dream in Nepal, even though this is the reality in places as politically distinct as Bhutan, Mongolia, and Tibetan regions of China.
Working with amchi on these clinics – including raising funds for them through DROKPA, an all-volunteer non-profit organization I co-founded in 1999 — has been one of the ways I’ve chosen to respond to the Nepal disasters as a medical anthropologist. I’m also incorporating younger amchi into collaborative research teams that will investigate responses to these events in three contiguous districts (Mustang, Manang, and Gorkha) through an NSF RAPID award of which I am a part.
I chose to open this blogpost with the words of Rudolf Virchow even though I know that he and many of Nepal’s amchi would see the relationship between what Virchow calls ‘faith’ and its relationship to medicine and science quite differently. Despite these epistemological divergences, I think they would all agree on fundamental premises of being of service and seeing the individual body as a microcosm of the larger social, ecological, and political worlds to which one belongs.
Heinrich Jäschke, a nineteenth-century Moravian missionary to Ladakh, is mostly known amongst scholars of Tibet for his pioneering 1881 Tibetan–English Dictionary. In his entry on ‘rlung’—a fundamental concept of Tibetan medicine and Tibetan Tantric Buddhism, commonly translated into English as ‘wind’ or ‘vital energy’—following his definition of the term, he added: ‘These notions concerning rlung are one of the weakest points of Tibetan physiology and pathology’. Strong words for a dictionary.
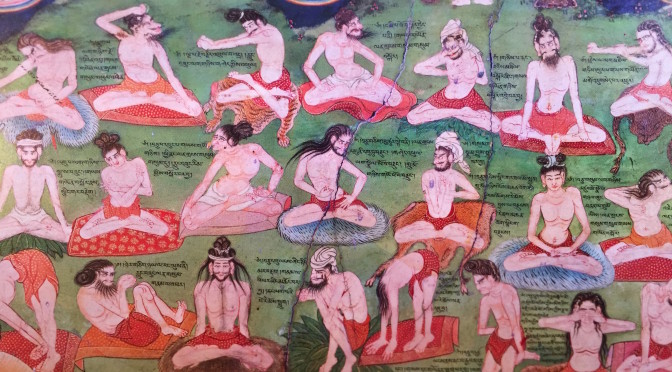
It is hard to think of what might better demonstrate the extent to which western perception of the term has evolved since Jäschke wrote those words than the new Wellcome exhibition “Tibet’s Secret Temple: Body, Mind and Meditation in Tantric Buddhism” which opened in London this week. The focus of this major exhibition is a series of intricate murals adorning the walls of the Lukhang (klu khang) Temple in Lhasa. Situated on a small island on a lake behind the Potala in Lhasa, the Lukhang was built in the late 17th century during the reigns of the Fifth and Sixth Dalai Lamas as a private sanctuary for meditation and spiritual practice.
One key focus of these murals is a fascinating depiction of a tradition of exercises known as trulkhor (‘khrul ‘khor or ‘phrul ‘khor), combining both physical movements and breathing, to stabilise and regulate one’s rlung. Rlung links between what in western terms is termed ‘body’ and ‘mind’. With its inherent crossing over between ‘body’ and ‘mind’, it is a concept that calls into our attention an awareness that the mere standard western interpretations of what constitutes ‘body’ and what constitutes ‘mind’ are largely irrelevant when trying to understand the Tibetan medical and Buddhist modes of understanding human beings.
Trulkhor practices, once only taught to advanced practitioners, are now increasingly practised and even used within conventional biomedical settings. Approaches to body-mind, well-being and meditation—all deriving from the Tibetan understanding of rlung—are more generally making their mark on western methods of treatments.
Even by Tibetan standards the Lukhang is pretty hard to get to. Of the eminent Tibetologists and Tibetophiles who assembled at the opening night, there were only less than a handful who ever managed to enter it. The intricate, thoughtful and sophisticated reconstruction of the murals in the exhibition has made them, not just more accessible, but also in many respects better than the originals. Every single posture is visible, every single caption is readable. But perhaps more importantly: the space in which they are reconstructed—and the process one goes through leading to that space—is profoundly inspirational. This is curating at its best.
Tibet’s Secret Temple: Body, Mind and Meditation in Tantric Buddhism runs at the Wellcome Collection, 183 Euston Road, London NW1 2BE, from 19 November 2015 to 28 February 2016.
Seventh International Congress on Traditional Asian Medicine (ICTAM VII)
September 7th to 11th, 2009
Institute for traditional medicine services, Thimphu, Bhutan
The International Association for the Study of Traditional Asian Medicine (IASTAM) meets every three years for an International Congress on Traditional Asian Medicine (ICTAM). Founded in 1979, IASTAM is the only international organisation in the field of Asian medicine making a serious attempt to embrace both academics and practitioners. It holds regional and international conferences (e.g. in Canberra in 1979, Surabaya in 1984, Bombay in 1990, Tokyo in 1994 and in Austin in 2006), publishes a regular newsletter, and produces the only peer reviewed academic journal in the field, Asian Medicine: Tradition and Modernity, published with Brill in Leiden.
The 2009 gathering of IASTAM, the Seventh Congress on Traditional Asian Medicine (ICTAM VII) was held in Thimphu, Bhutan, from September 7-11, 2009, hosted by the Institute for Traditional Medicine Services (ITMS), Royal Government of Bhutan.
The theme for the congress, ‘Asian Medicine: Cultivating Traditions and the Challenges of Globalization’, was positively received by both Bhutanese hosts and national and international participants enabling a wide variety of topics and issues being discussed. The congress brought about unique communications between scholars, scientists, policymakers and practitioner. We witnessed a growth in the range of topics and methodological approaches in the conferences’ schedule, from history, philology and religion to literature, Asian medical and biomedical practices and sciences, and from anthropology, art history, material culture, law to globalisation, gender studies and modernity.
With 200 participants in attendance, including practitioners and academics as well as private entrepreneurs and government civil servants from 30 countries, IASTAM as an organisation remains true to its ethos of being both international and interdisciplinary at its heart, as conceived of 30 years ago by Charles Leslie and A. L. Basham, the founders of IASTAM.
A collection of audio recordings from a panel on Himalayan medicine presented at the conference is available below.
#
Presenter
Subject
Date
Download.wma file
01
Calum Blaikie
“Critically Endangered? Himalayan Medicinal Plant Conservation and Diversity in Medical Cultures”
7 Sept 09
02
Carroll Dunham
“From Wild to Cultivated: Can Valued Sowa Rigpa Medicinal Plants Meet Market Demands Sustainably and Benefit Local Communities?”
7 Sept 09
03
Chamundeeswari Kuppuswamy
“The Ethics of Intellectual Property Rights: the Impact of Traditional Knowledge and Health”
7 Sept 09
04
Daniel Winkler
“Yartsa Gunbu (Cordyceps sinesis): An Ancient Medicinal Fungus Transforming Rural Tibet”
9 Sept 09
05
Dr Dawa
“Perspectives from the Tradition of Tibetan Medicines on the Nature, Identification, and Potencies of Organic Materia Medica, as well as their Protection and Increased Production’
7 Sept 09
n/a
06
Ed Smith
“Conservation of Wild Medicinal Plants Through Sustainable Wild-Harvesting and Propagation by Organic Agriculture Worldwide”
8 Sept 09
07
Gyatso Bista
“Conservation, Cultivation, and Sustainable Use of Medicinal Plants: Preliminary Report from Trials in Mustang, Nepal”
9 Sept 09
08
Herbert Schwabl
“Tibetan Medicine in the European OTC-Context”
9 Sept 09
09
Jan Salick
“Tibetan Medicine and Climate Change”
7 Sept 09
10
Kalden Nyima
“Endangered Tibetan Medicinal Plants and their Protection”
8 Sept 09
11
Kalden Nyima
“Medicinal Plants Conservation and Traditional Knowledge Transferring in Kawagebo Region”
9 Sept 09
12
Martin Saxer
“Recent Developments in Cross-border Trade of Tibetan Medicinal Plants”
8 Sept 09
13
Mona Schrempf
“Globalisation of Traditional Chinese and Tibetan Medicines between China and Europe: And Interdisciplinary Research Agenda”
7 Sept 09
14
panel discussion
10 Sept 09
15
Pei Shengji
“Medicinal Plants and Conservation in China with Reference in Chinese Himalayan Region”
9 Sept 09
16
Sonam Dorje
“To Treasure Wild Medicinal Plant Resources and Conserve Tibetan Culture”
7 Sept 09
17
Tsewang Gonbo
“An Alternative Approach to Medicinal Plant Conservation in Ladakh, India”
9 Sept 09
n/a
18
Ugyen Dorji
“Medicinal Plants and Their Conservation in Bhutan”